A 22 yr old female who is a student came with complaints of generalized weakness and easy fatiguability since 2 months
History of Presenting illness
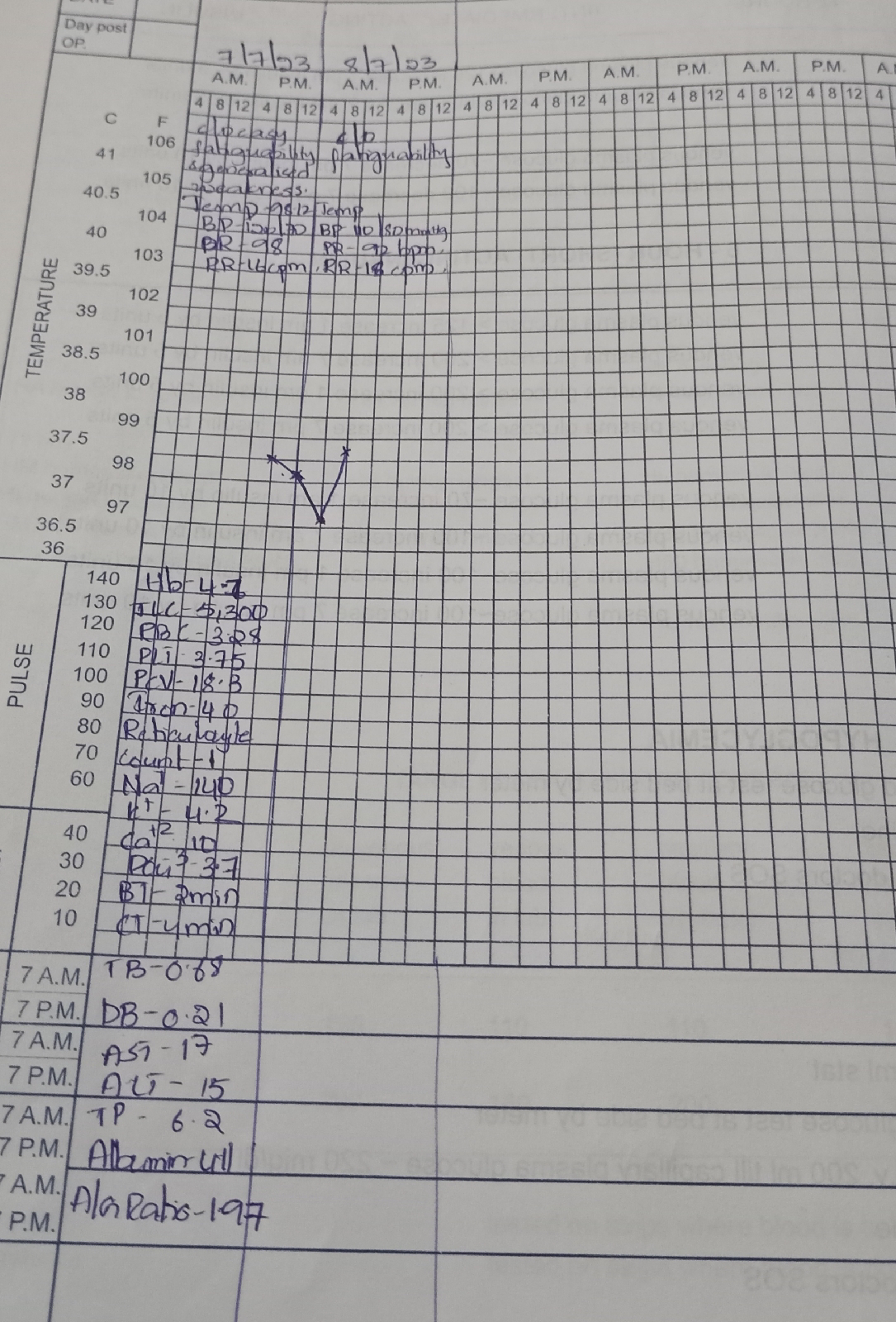
Pt was apparently asymptomatic 5 years back then she started to have desire to eat non edible material and went to the hospital and was diagnosed with Anemia (Hb 4gm/dl) and 2 units of PRBC transfusion was done
Now since 2 months she is complaining of easy fatiguability with generalized weakness
C/o SOB(grade ll-III) insidious in onset, gradually progressive to grade III,c/o exertional dyspnea
No c/o chest pain, palpitations, orthopnea,pnd
No c/o fever,loose stools, vomitings
PAST HISTORY
H/o similar complaints in the past
H/o two PRBC transfusion
N/k/c/o diabetes HTN TB Asthma Epilepsy thyroid disorders
PERSONAL HISTORY
Diet Mixed
Appetite normal
Sleep adequate
Bowel and bladder regular
Addictions No
Daily routine
Pt wakes up around 7 am takes breakfast and goes for coaching institute and comes back at 6 am and takes dinner at 8 pm and sleeps around 10 pm
Her daily routine did not changed even after the illness
General Examination
Pt is conscious coherent and cooperative
Pallor present
No Icterus, cyanosis, clubbing generalized lymphadenopathy,edema
Vitals
Temp afebrile
Bp 110/80 mm Hg
PR 92 bpm
RR
Systemic Examination
Cardiovascular system
Inspection :
Shape of chest- Normal
No engorged veins, scars, visible pulsations
Palpation :
Apex beat can be palpable in 5th inter costal space medial to mid clavicular line
No thrills felt
Auscultation :
S1,S2 are heard
No Murmurs
Inspection -
Umbilicus - inverted
All quadrants moving equally with respiration
No scars, sinuses and engorged veins , visible. pulsations.
Hernial orifices- free.
Palpation -
soft, non-tender
no palpable spleen and liver
Percussion:Resonant note heard
Auscultation- normal bowel sounds heard
Respiratory system
Bilateral entry present
Normal vesicular breath sounds heard
CNS NFD




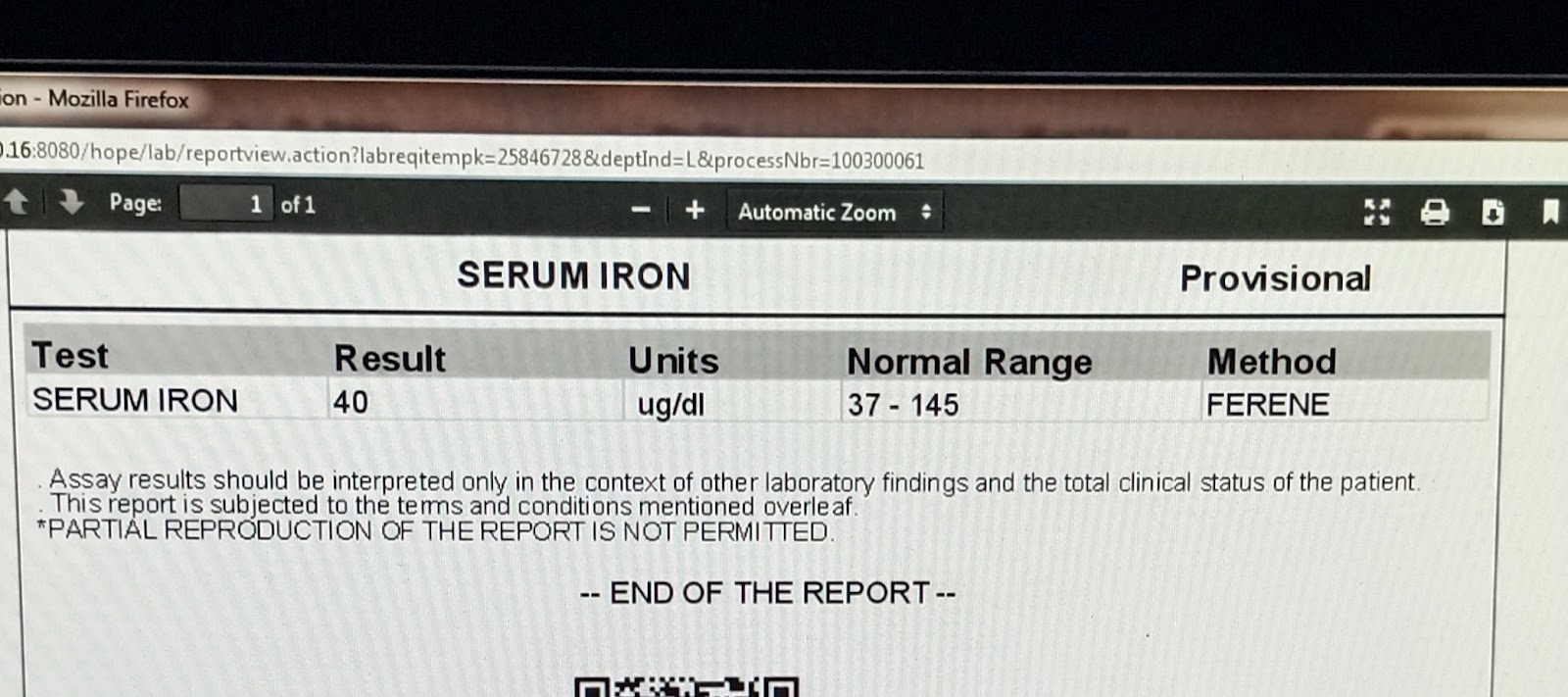











DIAGNOSIS
IRON DEFICIENCY ANEMIA in
8/07/2023
1 PRBC transfusion done
Hb 7.6
10/7/2023
1 PRBC transfusion done
Comments
Post a Comment